Bionic Ear

A cochlear implant (CI) is a surgically implanted electronic device that provides a sense of sound to a person who is profoundly deaf or severely hard of hearing. Cochlear implants are often called bionic ears.
Cochlear implants may help provide hearing in patients that are not deaf because of damage to sensory hair cells in their cochleas. In those patients, the implants often can enable sufficient hearing for better understanding of speech. The quality of sound is different from natural hearing, with less sound information being received and processed by the brain. However, many patients are able to hear and understand speech and environmental sounds. Newer devices and processing-strategies allow recipients to hear better in noise, enjoy music, and even use their implant processors while swimming.
As of December 2010, approximately 219,000 people worldwide have received cochlear implants; in the U.S., roughly 42,600 adults and 28,400 children are recipients.The vast majority are in developed countries due to the high cost of the device, surgery and post-implantation therapy. A small but growing segment of recipients have bilateral implants for hearing stereo sound (one implant in each cochlea).[9]
Cochlear implants may help provide hearing in patients that are not deaf because of damage to sensory hair cells in their cochleas. In those patients, the implants often can enable sufficient hearing for better understanding of speech. The quality of sound is different from natural hearing, with less sound information being received and processed by the brain. However, many patients are able to hear and understand speech and environmental sounds. Newer devices and processing-strategies allow recipients to hear better in noise, enjoy music, and even use their implant processors while swimming.
As of December 2010, approximately 219,000 people worldwide have received cochlear implants; in the U.S., roughly 42,600 adults and 28,400 children are recipients.The vast majority are in developed countries due to the high cost of the device, surgery and post-implantation therapy. A small but growing segment of recipients have bilateral implants for hearing stereo sound (one implant in each cochlea).[9]
History
The discovery that electrical stimulation in the auditory system can create a perception of sound occurred around 1790.
The first direct stimulation of an acoustic nerve with an electrode was performed in the 1950s by the French-Algerian surgeons André Djourno and Charles Eyriès. They placed wires on nerves exposed during an operation, and reported that the patient heard sounds like "a roulette wheel" and "a cricket" when a current was applied.
The first attempt to develop a clinical CI was in 1957 by Djourno and Eyriès. A recipient was implanted with a single channel device. Unprocessed sounds were transmitted via a pair of solenoid-like coils. The link was therefore transcutaneous; it did not require a break in the skin after implantation. This device failed after a short time and another device was implanted. After this second device failed, Eyriès refused to implant a third device. He urged Djourno to collaborate with an industry partner to build a more reliable device. Djourno refused because he believed that academia should not be tainted by commerce. Djourno found another surgeon, Roger Maspétiol, who implanted a second patient in 1958. Although these recipients were unable to understand speech with the device alone, it helped with lipreading by providing the rhythm of the speech.
In 1961, Dr. William F. House, an otologist considered the inventor of the cochlear implant, John Doyle (a neurosurgeon) and James Doyle (an electrical engineer) commenced work on a single-channel device in Los Angeles. In one case a five-wire electrode was used but the same signal was applied to all contacts. House’s work continued in the 1970s in collaboration with engineer Jack Urban. Their implant was also a single-channel device but, in this case, the speech was modulated onto a carrier of 16 kHz.
In 1964, Blair Simmons at Stanford University implanted some recipients with a six-channel device. This device used a percutaneous plug to enable the electrodes to be individually stimulated. Recipients could still not understand speech through the device but, importantly, it demonstrated that by stimulating in different areas of the cochlea, different pitch percepts could be produced.
In 1970, Robin Michelson, M.D., reported preliminary results of cochlear implantation in three deaf adults implanted with gold wire electrodes. Initially he teamed with Mel Bartz, an electrical engineer working with Storz, Inc. Michelson's report to the American Academy of Otolaryngology and Ophthalmology created a tempest. Orthodox auditory theory was in confusion at the time, and it was not thought possible for direct electrical stimulation of neural tissue to convey meaningful sound to the brain. Michelson conducted some work in San Francisco, in the Coleman Laboratory at the University of California. Michelson's implantation of humans before animal physiology experiments caused consternation among physiologists, audiologists, and many otologists. An otolaryngology resident, C. Robert Pettit, heard Michelson describe the results of his cochlear implantations at a department educational meeting. He ran to the Coleman Laboratory, where Michelson spent one half-day per week away from his Redwood City private ENT practice, and told the older surgeon of his dream since college of a multi-channel electrode resembling a hairbrush. Michelson said so many stimulus points were not necessary and that his patients were hearing "in stereo" with a two-channel electrode he had designed. Michelson and Pettit teamed to build the bipolar electrodes embedded in silastic which replaced the broken gold electrodes in Michelson's three patients. The reimplantation procedures were carried out in Redwood City Community Hospital, not at UC San Francisco, as were the original implants.
In 1972, a version of "Where Have All the Flowers Gone?" played on a Moog Synthesizer was presented to the patient through the cochlear implant. The camera caught the patient humming the melody and tapping a pencil to the tempo of the tune. That sequence convinced the department chairman to support the cochlear implant project. When the film was shown to a meeting of otologists later in 1972, it convinced the scientific community that meaningful sound could be conveyed to the brain by electrical stimulation of the auditory nerve.
Cochlear implants that operate successfully, including those produced by all three major manufacturers (Cochlear Corporation, Advanced Bionics and Med-El), incorporate the same basic design. Likewise, all cochlear implants incorporate the same basic design to be capable of the ultimate goal of "detecting" or "demodulating" intelligence from the human voice when that intelligence is residing within an electronic signal. The successful cochlear implant must also be capable of converting the pattern of the detected intelligence into an appropriate electronic format for application to the acoustic (eighth cranial) nerve, which in turn further transmits the encoded pattern to the hearing center of the brain, where the information is interpreted as meaningful intelligence. That is why implants from all (three) major manufacturers work equally well in functionality, but are quite different in final design enhancements.
Some cochlear implant designs and intra-cochlear implantations were made prior to the mid-1970s, and were considered "successful" from a surgical and medical point of view. An equal number of proclamations and claims of being "firsts" in cochlear implantation were also made. Indeed, many important advances in cochlear implantation were accomplished during the 1960s and '70s. These earlier implants were capable of providing background sounds, and provided some aid to lip reading, and thus enabled patients to attain a most welcome sense of "attachment" to the world of sound. These earlier implants were incapable, however, of providing the ultimate level of comprehension of the intelligence of the spoken human voice enjoyed by the implant users of today. This fact can be supported by review of the many volumes of quarterly reports provided by many researchers under contract to the National Institutes of Health.
In 1976 a paper (received Feb 1975) was published by Pialoux, Chouard and McLeod that stated that, in the six months before the paper's submission, seven patients were implanted with an eight-channel device.Although it was reported that about 50% of ordinary words were understood without lipreading, this has not been supported by audiological data in the literature.
In 1972 the House 3M single-electrode implant was the first to be commercially marketed.However, it was Dr. Michelson's patents and ultimately device which are thought of as the first cochlear implants.
Parallel to the developments in California, in the 1970s there were two other groups working on the development of the cochlear implant in Vienna, Austria, and Melbourne, Australia. On December 16, 1977, professor Kurt Burian implanted a multichannel cochlear implant. The device was developed by the scientists Ingeborg and Erwin Hochmair, who founded MED-EL, producer of hearing implants, in 1989.
Professor Graeme Clark A.C., then Foundation Professor of the Department of Otolaryngology at the University of Melbourne in 1970, led the team that developed the Australian prototype bionic ear, which was implanted into the first patient, Rod Saunders, in 1978.
In December 1984, the Australian cochlear implant was approved by the United States Food and Drug Administration to be implanted in adults in the United States. In 1990 the FDA lowered the approved age for implantation to two years, then 18 months in 1998, and finally 12 months in 2000, although off-label use has occurred in babies as young as 6 months in the United States and 4 months internationally.
Throughout the 1990s, the large external components which had been worn strapped to the body grew smaller and smaller, thanks to developments in miniature electronics. By 2006, most school-age children and adults used a small behind-the-ear (BTE) speech processor about the size of a power hearing aid. Younger children have small ears and might mishandle behind-the-ear speech processors, therefore, they often wear the sound processor on their hip in a pack or small harness or wear the BTEs pinned to their collar, barrette or elsewhere.
In 1991, the systems changed from being converted through an analog compressor, now became digital. On October 5, 2005, the first of three recipients was implanted with Cochlear's TIKI device, a totally implantable cochlear implant, in Melbourne, Australia. This was part of a research project conducted by Cochlear Ltd and the University of Melbourne Department of Otolaryngology under the umbrella of CRC HEAR to be the first cochlear implant system capable of functioning for sustained periods with no external components. The system is capable of providing hearing via the TIKI device in stand-alone mode (invisible hearing) or via an external sound processor. Although these recipients continue to use their devices successfully today, it will be many years before a commercial product becomes available.
Since hearing in two ears allows people to localize sounds (given synchronised AGCs) and to hear better in noisy environments, bilateral (both ear) implants are being investigated and used. Users generally report better hearing with two implants, and tests show that bilateral implant users are better at localizing sounds and hearing in noise.However, there is also evidence to suggest that the combination of one implant with an FM system provides better speech recognition in noise than two implants alone.Additionally, dynamic FM technology has been proven to outperform traditional FM when used with cochlear implants.
Nearly 3,000 people worldwide are bilateral cochlear implant users, including 1,600 children.As of 2006, the world's youngest recipient of a bilateral implant was just over 5 months old (163 days) in Germany (2004).
The first direct stimulation of an acoustic nerve with an electrode was performed in the 1950s by the French-Algerian surgeons André Djourno and Charles Eyriès. They placed wires on nerves exposed during an operation, and reported that the patient heard sounds like "a roulette wheel" and "a cricket" when a current was applied.
The first attempt to develop a clinical CI was in 1957 by Djourno and Eyriès. A recipient was implanted with a single channel device. Unprocessed sounds were transmitted via a pair of solenoid-like coils. The link was therefore transcutaneous; it did not require a break in the skin after implantation. This device failed after a short time and another device was implanted. After this second device failed, Eyriès refused to implant a third device. He urged Djourno to collaborate with an industry partner to build a more reliable device. Djourno refused because he believed that academia should not be tainted by commerce. Djourno found another surgeon, Roger Maspétiol, who implanted a second patient in 1958. Although these recipients were unable to understand speech with the device alone, it helped with lipreading by providing the rhythm of the speech.
In 1961, Dr. William F. House, an otologist considered the inventor of the cochlear implant, John Doyle (a neurosurgeon) and James Doyle (an electrical engineer) commenced work on a single-channel device in Los Angeles. In one case a five-wire electrode was used but the same signal was applied to all contacts. House’s work continued in the 1970s in collaboration with engineer Jack Urban. Their implant was also a single-channel device but, in this case, the speech was modulated onto a carrier of 16 kHz.
In 1964, Blair Simmons at Stanford University implanted some recipients with a six-channel device. This device used a percutaneous plug to enable the electrodes to be individually stimulated. Recipients could still not understand speech through the device but, importantly, it demonstrated that by stimulating in different areas of the cochlea, different pitch percepts could be produced.
In 1970, Robin Michelson, M.D., reported preliminary results of cochlear implantation in three deaf adults implanted with gold wire electrodes. Initially he teamed with Mel Bartz, an electrical engineer working with Storz, Inc. Michelson's report to the American Academy of Otolaryngology and Ophthalmology created a tempest. Orthodox auditory theory was in confusion at the time, and it was not thought possible for direct electrical stimulation of neural tissue to convey meaningful sound to the brain. Michelson conducted some work in San Francisco, in the Coleman Laboratory at the University of California. Michelson's implantation of humans before animal physiology experiments caused consternation among physiologists, audiologists, and many otologists. An otolaryngology resident, C. Robert Pettit, heard Michelson describe the results of his cochlear implantations at a department educational meeting. He ran to the Coleman Laboratory, where Michelson spent one half-day per week away from his Redwood City private ENT practice, and told the older surgeon of his dream since college of a multi-channel electrode resembling a hairbrush. Michelson said so many stimulus points were not necessary and that his patients were hearing "in stereo" with a two-channel electrode he had designed. Michelson and Pettit teamed to build the bipolar electrodes embedded in silastic which replaced the broken gold electrodes in Michelson's three patients. The reimplantation procedures were carried out in Redwood City Community Hospital, not at UC San Francisco, as were the original implants.
In 1972, a version of "Where Have All the Flowers Gone?" played on a Moog Synthesizer was presented to the patient through the cochlear implant. The camera caught the patient humming the melody and tapping a pencil to the tempo of the tune. That sequence convinced the department chairman to support the cochlear implant project. When the film was shown to a meeting of otologists later in 1972, it convinced the scientific community that meaningful sound could be conveyed to the brain by electrical stimulation of the auditory nerve.
Cochlear implants that operate successfully, including those produced by all three major manufacturers (Cochlear Corporation, Advanced Bionics and Med-El), incorporate the same basic design. Likewise, all cochlear implants incorporate the same basic design to be capable of the ultimate goal of "detecting" or "demodulating" intelligence from the human voice when that intelligence is residing within an electronic signal. The successful cochlear implant must also be capable of converting the pattern of the detected intelligence into an appropriate electronic format for application to the acoustic (eighth cranial) nerve, which in turn further transmits the encoded pattern to the hearing center of the brain, where the information is interpreted as meaningful intelligence. That is why implants from all (three) major manufacturers work equally well in functionality, but are quite different in final design enhancements.
Some cochlear implant designs and intra-cochlear implantations were made prior to the mid-1970s, and were considered "successful" from a surgical and medical point of view. An equal number of proclamations and claims of being "firsts" in cochlear implantation were also made. Indeed, many important advances in cochlear implantation were accomplished during the 1960s and '70s. These earlier implants were capable of providing background sounds, and provided some aid to lip reading, and thus enabled patients to attain a most welcome sense of "attachment" to the world of sound. These earlier implants were incapable, however, of providing the ultimate level of comprehension of the intelligence of the spoken human voice enjoyed by the implant users of today. This fact can be supported by review of the many volumes of quarterly reports provided by many researchers under contract to the National Institutes of Health.
In 1976 a paper (received Feb 1975) was published by Pialoux, Chouard and McLeod that stated that, in the six months before the paper's submission, seven patients were implanted with an eight-channel device.Although it was reported that about 50% of ordinary words were understood without lipreading, this has not been supported by audiological data in the literature.
In 1972 the House 3M single-electrode implant was the first to be commercially marketed.However, it was Dr. Michelson's patents and ultimately device which are thought of as the first cochlear implants.
Parallel to the developments in California, in the 1970s there were two other groups working on the development of the cochlear implant in Vienna, Austria, and Melbourne, Australia. On December 16, 1977, professor Kurt Burian implanted a multichannel cochlear implant. The device was developed by the scientists Ingeborg and Erwin Hochmair, who founded MED-EL, producer of hearing implants, in 1989.
Professor Graeme Clark A.C., then Foundation Professor of the Department of Otolaryngology at the University of Melbourne in 1970, led the team that developed the Australian prototype bionic ear, which was implanted into the first patient, Rod Saunders, in 1978.
In December 1984, the Australian cochlear implant was approved by the United States Food and Drug Administration to be implanted in adults in the United States. In 1990 the FDA lowered the approved age for implantation to two years, then 18 months in 1998, and finally 12 months in 2000, although off-label use has occurred in babies as young as 6 months in the United States and 4 months internationally.
Throughout the 1990s, the large external components which had been worn strapped to the body grew smaller and smaller, thanks to developments in miniature electronics. By 2006, most school-age children and adults used a small behind-the-ear (BTE) speech processor about the size of a power hearing aid. Younger children have small ears and might mishandle behind-the-ear speech processors, therefore, they often wear the sound processor on their hip in a pack or small harness or wear the BTEs pinned to their collar, barrette or elsewhere.
In 1991, the systems changed from being converted through an analog compressor, now became digital. On October 5, 2005, the first of three recipients was implanted with Cochlear's TIKI device, a totally implantable cochlear implant, in Melbourne, Australia. This was part of a research project conducted by Cochlear Ltd and the University of Melbourne Department of Otolaryngology under the umbrella of CRC HEAR to be the first cochlear implant system capable of functioning for sustained periods with no external components. The system is capable of providing hearing via the TIKI device in stand-alone mode (invisible hearing) or via an external sound processor. Although these recipients continue to use their devices successfully today, it will be many years before a commercial product becomes available.
Since hearing in two ears allows people to localize sounds (given synchronised AGCs) and to hear better in noisy environments, bilateral (both ear) implants are being investigated and used. Users generally report better hearing with two implants, and tests show that bilateral implant users are better at localizing sounds and hearing in noise.However, there is also evidence to suggest that the combination of one implant with an FM system provides better speech recognition in noise than two implants alone.Additionally, dynamic FM technology has been proven to outperform traditional FM when used with cochlear implants.
Nearly 3,000 people worldwide are bilateral cochlear implant users, including 1,600 children.As of 2006, the world's youngest recipient of a bilateral implant was just over 5 months old (163 days) in Germany (2004).
Parts of the cochlear ear
- one or more microphones which picks up sound from the environment
- a speech processor which selectively filters sound to prioritize audible speech, splits the sound into channels and sends the electrical sound signals through a thin cable to the transmitter,
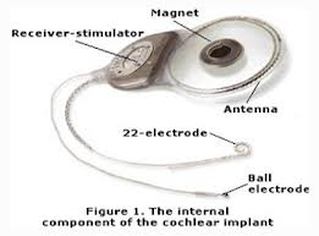
- a transmitter, which is a coil held in position by a magnet placed behind the external ear, and transmits power and the processed sound signals across the skin to the internal device by electromagnetic induction,
- a receiver and stimulator secured in bone beneath the skin, which converts the signals into electric impulses and sends them through an internal cable to electrodes,
- an array of up to 22 electrodes wound through the cochlea, which send the impulses to the nerves in the scala tympani and then directly to the brain through the auditory nerve system. There are 4 manufacturers for cochlear implants, and each one produces a different implant with a different number of electrodes. The number of channels is not a primary factor upon which a manufacturer is chosen; the signal processing algorithm is also another important block.
